


The lockdown in reaction to the Covid-19 pandemic will have terrible consequences on an informal economy that relies first and foremost on movements and will deepen the socioeconomic inequalities that divide the country. The risk of people dying from hunger is extremely high and the death toll worsened by poor health infrastructures.
Dossier / Faces of the Pandemic
The Covid-19 Crisis in India
A Nascent Humanitarian Tragedy
by
&
&
&
,
13 April 2020
|
In December, while Wuhan province was witnessing the beginning of the actual Covid-19 pandemic, India was facing massive and violent uprisings. Hundreds of thousands of Indians protested all over the country against the discriminatory anti-Muslim citizenship law that had just been passed by its parliament—the Citizenship Amendment Act (CAA)—and as a backlash violent attacks occurred on universities and Muslim working-class neighbourhoods by armed vigilantes. All this while the authorities were negating the presence of community transmission of the virus despite the first cases appearing way back in January to finally declare a 21-day lockdown on the midnight of 24 March, with only a 4 hour notice. This announcement, as in France, has triggered migration from the cities to the countryside, but of a completely different nature: in India, the internal migrant workers, day labourers and the poor—deprived of resources—have decided to return to their native villages. This tragic and deadly exodus of migrants fleeing cities is the most visible stigmata of the profound health, economic and social crisis that this threefold essay offers to analyse.
Accessing Healthcare under the Lockdown
This pandemic has brutally exposed the vulnerabilities of some of the best health systems. For the Indian health system, one of the most burdened and least funded in the world, this could be a critical moment; as government facilities are already overstretched in a highly fractured, underfunded and geographically uneven health system (Das 2015; Drèze & Sen 2013; Hodges & Rao 2016). This invites us to examine the way the current crisis risks to enhance long lasting health inequalities and how dysfunctional health infrastructures may collapse under the strain of the coming dramatic spike in Covid-19 cases in India.
Testing is crucial to gauge the extent of Covid-19 transmission in any country. India currently has one of the lowest ratios of testing in the world, which may have masked coronavirus cases. As of March 23rd, the total number of individuals tested for Covid-19 across the country was 17,493. The same week, South Korea was carrying out more than 5,500 tests per million people, Italy 2,500 per million, the United Kingdom close to 1,500 and France around 900. Even if the epidemic outbreak was ahead in these countries, India lags at just 10 tests per million. Until the national lockdown, the testing strategy of the government was relying on the assumption that no community transmission was happening in India, and that there were only foreign imported cases. Basing the testing strategy on this and testing only people coming from infected areas abroad may have unintended consequences on the spreading of the epidemic. Indeed, with the lockdown, a large amount of workers migrated internally from existing hotspots like Mumbai and Delhi towards their home states like Uttar Pradesh and Bihar. Failure to acknowledge presence of Covid-19 infections in the community and failure to test all symptomatics in Mumbai or Delhi itself may have exposed these states to the diffusion of the virus and a potential explosion of cases, in places where health infrastructures are poorer.
At the beginning of its national lockdown, India simply did not have enough testing kits and even if the government has given licenses to private companies to sell them in India, the constraint on testing lies in the number of laboratories. On 23rd of March, India had 118 accredited labs for a population of 1.3 billion with huge geographical inequalities; Arunachal Pradesh (1,5 million) and Nagaland (3,3 million) had no testing centres, Bihar had only one accredited lab for a population of 110 million compared to 8 facilities in Rajasthan for a population of 80 million. Even if states were supplied with an infinite number of testing kits, government labs would not be able to utilise them, as their testing capacity is around 90 samples per day. That’s why the government had allowed private players to conduct Covid-19 tests, which means that even those who are not hospitalised can get tested but at their own cost. The price cap of 4500 INR (around 55 euros) per test by the government, is too high for most Indians. With stigma associated with the virus and the actual lockdown some accredited private labs have already declared that the task was just impossible. Considering the high price of private testing and all the logistical problems associated with the lockdown, most Indians are likely to depend only on the public system to get tested. In an already stretched and underfunded public healthcare system, money spent on the coronavirus tests leaves less for other public health problems as India spends only 3.7 percent of its total budget on health. A budget that is far too limited to respond to the massive need of intensive care that has been necessary in countries already impacted by Covid-19.
If India has a lower proportion of elderly than other countries, its government healthcare facilities are limited and disproportionately burdened with patients having comorbidities—such as undernutrition, tuberculosis, diabetes, chronic respiratory and cardiovascular diseases [1]—that could aggravate the Covid-19 death toll for India. Among all infected people, the death rate is hovering at around one to three per cent, but among the critically ill, it climbs as high as 62 per cent. Most deaths are due to hypoxia, an insufficient supply of oxygen to the body’s tissues, or multi-organ collapse. Around five per cent of the infected patients in India will require intensive care and half of those admitted in the intensive care unit will require mechanical ventilation; up to 1 million ventilators at the peak of the Covid-19 epidemic may be needed. As per Ministry of Health estimates, as of March 24th there were 8432 ventilators in public hospitals, a number that could reach 50 000 if we factor in private hospitals. Compared to this, USA, which is currently overwhelmed with a Covid-19 outbreak, has 160 000 ventilators for a population that is one third of India. So far, India imports almost 75% of ventilators, its domestic production capacity stands at 5000 ventilators per month and also depends—for a few critical components—on international suppliers, who are all overstretched right now. Even the meagre numbers quoted above hide extreme disparities in access. Intensive care facilities, specially mechanical ventilation are concentrated in big urban areas and richer provinces; Mumbai alone has 1000 ventilators and Kerala 5000, which means there are a significantly lesser number of ventilators available in some of the poorest and most rural provinces of the country.
Same disparities will apply for intensive care beds, as hospital beds per 1000 population for 12 poorer states in India (70% of India’s population) are lower than the national average which stands at 0,7 bed per 1000 (compared to 11,5 in South Korea, 6,5 in France and 3,5 in Italy). [2] Even by most conservative estimates, 75% of Indian provinces will run out of beds for coronavirus patients by June. [3] Knowing that the average cost of private hospitalization in 2017 was Rs. 31845 ( 384 euros), that India’s monthly per capita income stands at Rs. 11254 ( 135 euros) and that a majority of Indians do not have any health insurance: [4] how many of the ailing patients will be able to afford private care, once the modest public facilities will be overwhelmed?
Given the severe challenges faced by the public health system and the dominance of unaffordable private health care in many Indian States, the response to the Covid-19 crisis must prioritize the strengthening of an affordable and accessible health care system for all, whether rich or poor, Hindu or Muslim, from Bihar or Kerala. But this pandemic also revealed the extreme and appalling vulnerability of most Indians to a catastrophe that goes far beyond healthcare. In addition, and far beyond the risk of infection, the measure taken to contain contagions—the lockdown—will also have disastrous consequences for a large part of the population.
Making a Living under the Lockdown
What does “lockdown” mean in a context where people, not just the poorest, depend on mobility and sociability to make a living? Using culturalist clichés, many media have highlighted the “cultural” difficulty of accepting the principle of social distancing. Long before being a “cultural” issue, and if this argument is valid, in economies where informal employment is the rule rather than the exception, and where social protection remains the privilege of a minority, social connection and movement are simply necessary for survival and protection.
India is characterized by the extent of informal employment. According to ILO statistics, 92% of jobs are informal in the sense that they exclude any form of protection, contract and guarantee of continuity (ILO 2016). India is also characterized by the crucial role of internal migration and circulation (Breman 2007; Picherit 2018). Largely underestimated by official statistics, these displacements give rise to various estimates of up to 100 million workers (Deshingkar and Akter 2009). While these workers’ movements have always existed, they have undoubtedly increased to meet the needs of a capitalist economy always in search of cheap and disciplined labour. Internal migration includes long-distance, inter-state migration, with massive flows from the poorest states in north-eastern India to the most employment-intensive states located in the west and south. Internal migration also includes short term forms of commuting from villages to nearby towns. With the massive decline in agriculture in recent decades, [5] and even as India resists the rural exodus, many villagers survive by moving daily to nearby urban centres. Some of these migrants settle in cities, swelling the miserable mass of slums, but most remain attached to their home villages. The Indian labour force, and men in particular, is thus caught in a continuous flow, moving with the seasons and years according to opportunities, networks, and above all the needs of the capitalist system, while regularly returning home. The latter remains the pivot of family and village roots and identity.
Movement is not just about finding jobs. These generate incomes that are both low and unpredictable. At the same time, households face incompressible and ever-increasing expenses: eating; [6] maintaining housing, often precarious and therefore requiring constant renovation and improvement; sending children to school; [7] charges for electricity, sometimes water and gas; social and religious rituals; [8] durable consumer goods that are now required, including for work (mobile phones, two-wheeled motor vehicles). To these regular and incompressible expenses are added unforeseen expenses: health shocks, sudden loss of a job, legal fees, theft, seizure of land following a conflict or an unpaid debt and so forth.
To cope with this mismatch between income flows and expenditures, individuals, both men and women, mobilize complex portfolios of financial practices in which debt is central. Savings are not completely absent, but among the poorest and for a large part of the rural population, they rarely take the form of monetary savings. Jewels, grains, livestock, as well as “social investments” (reciprocal gifts or loans) are much more common. Any surplus liquidity is often reinjected into the social network.
Debt is thus a central component of daily survival. Yet debt implies movement and sociability, either on the part of a family member who has to move to meet a lender, or on the part of a financial provider, since some provide doorstep services. Financial diary methods, aimed at tracing all of a household’s financial flows over a given period, confirm the intensity of movements related to financial transactions. This is even more true for women, since they are often the ones in charge of managing family budgets. A survey of this type conducted in 2017-2018 in the states of Pondicherry and Tamil Nadu shows that the number of transactions (borrowing, repaying, lending, getting repaid, giving, receiving) can reach peaks of 30 transactions per week for women, 20 for men (Reboul et al., 2019).
Given the crucial importance of movement and sociability, we can therefore imagine that the lockdown will have absolutely devastating consequences, and it already has. The invisibility of migrant workers, a vital link in India’s economy, has become glaringly apparent. They have simply been ignored by the lockdown measures. Prime Minister Narendra Modi’s announcement of “stay home” provoked a massive influx of workers desperate to return home, even though transport infrastructure had already been drastically reduced. Testimonies collected over the first weeks of the lockdown in Tamil Nadu attest to widespread panic. The populations are used to shocks—the Tsunami in 2004, the demonetization in 2016 [9]—but the announcement of the lockdown seems much more frightening to them.
Tamil migrants have returned. Not only do they have no job prospects, but some are already heavily in debt. In some sectors, such as brick molding or sugar cane cutting, recruitment and control of the workforce is based on a wage advance. This advance is usually repaid over the course of the season, depending on the productivity of the workers. Since the season had barely started (January), most of these migrants find themselves with a debt of 70,000 to 100,000 INR (6 to 8 months’ salary for two workers). It remains to be seen whether employers and labour recruiters will agree to wipe out some of this debt. As for local workers, the sources of debt, a condition for their daily survival, have dried up. While usually the slightest surplus is lent or given away, what is observed at present is a complete withdrawal. From landowners to housewives, all testimonies converge: given the prevailing uncertainty, everyone tends to keep their stocks, whether it is cash or grain. Some farmers have offered wage payments in kind to their labour (mostly female), who in turn find it difficult to convert into cash.
Conversely, lenders demand their due and refuse to lend. The Reserve Bank of India has announced a moratorium regarding the suspension of loan repayments. But this does not concern small financial companies, even though they are the ones that target the poor. Those companies keep on sending messages and oral instructions to borrowers in order to enforce repayments. Nationalized banks and some finance companies allow the suspension, but borrowers have to fill the specific online forms that are not accessible for many of them, especially when borrowers are poor rural women. This moratorium applies even less to informal lenders. In such a context, how do people manage? For now, they are “adjusting”, as we were told. They are drawing on the few savings available. While monetary savings are limited, many families, often through women, have a few hundred or even a few thousand rupees secretly hidden and intended to cope in case of a hard blow. They save on food. But this coping strategy is not sustainable.
Dying of Hunger under the Lockdown
Upon the lockdown announcement, middle class Indians were seen rushing to shops and markets to buy food provisions. This was particularly triggered by the lack of official preparation to reassure people that they would still be able to access food shops under the lockdown. [10] But others simply did not have advance funds to save food and the phrase “I won’t die of corona. Before that, I will surely die of hunger” crudely summarizes many poor’s precarious condition. For any economic shock, the lack of savings and the high share of food in total spending are two ingredients of a nascent humanitarian tragedy. Looking at food security reveals how vulnerable Indian households are. The average share of food in household total spending amounts to 43 percent in urban India and rises to 53 percent in rural India. [11] As a point of comparison, French households spent about 20 percent of their total expenditures in food and beverages in 2014. [12] Besides according to Engel’s law, the poorer a household, the larger the share of total expenditures spent on food. Indian 5 percent poorest households in rural areas dedicate about 61 percent of their total spending to food, while in urban areas, this share was only 28 percent for the 5 percent richest. Any economic shock is very likely to impact access to food, particularly among the poor.
In the present context, economic consequences on food are expected from two mechanisms. The first and most dangerous one is for all households losing their source of income. With little savings, those households who belong to the poorest segments of society are the first affected by the situation, among which the daily-wage earners, and more especially urban migrants, who are often left without any resource or even shelter. A second expected effect will affect all segments of society: the chain of food supply may not sustain itself. Some shopkeepers fear to open their shops, and street hawkers are not allowed to sell their stock. Mobility has been severely hampered and hence food procurement is disrupted. [13] On the production side, the lack of mobility of agricultural labourers endangers the harvest. [14] Therefore difficulties in the supply of provisions may create food shortages and already increase food prices, against which the government now intervenes to set up price caps on necessary items.
First reports of hunger crises cannot let anyone indifferent: in Bihar, an 8-year-old kid died of hunger just six days after the lockdown started. More cases are unfortunately awaited given India’s nutritional situation, characterized by chronic malnutrition (lack of food balance) and to some extent by acute malnutrition (a visible form of undernutrition). According to the latest 2019 estimates, India ranked 102 out of 117 countries on the Global Hunger Index, the lowest among South Asian countries (despite higher GDP per capita). [15] The 2019 edition of the State of the World’s Children from UNICEF points the enduring problem of hunger in India: about half of all deaths among children under 5 are attributable to undernutrition. Child underweight, measured as ‘weight-for-age’, which entails aspects of both chronic and acute malnutrition, was at a 36 per cent high in 2015-2016 (the World Health Organization considers that a level of underweight higher than 30 percent reflects a “very high prevalence”). [16] These figures conceal important regional and socioeconomic disparities (Swaminathan et al., 2019). Underweight is noticeably higher in North Central and especially Eastern states of India (see map): in Jharkhand (48 percent), Bihar (44 percent), but nothing compared to Kerala (16 percent). Clearly, some regions face a heightened burden in the present lockdown.
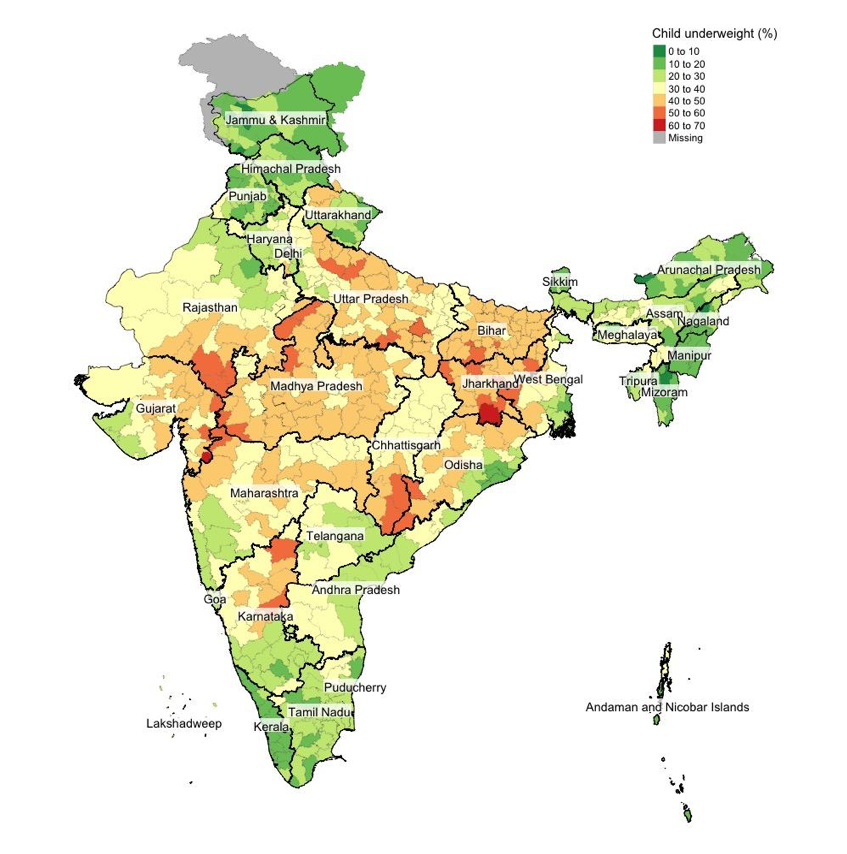
Regional disparities in child underweight in India.
Note: the figures are computed from the National Family Health Survey 4 (2015-2016) and are plotted by district. Child underweight is computed following the definition: weight for age < –2 standard deviations (SD) of the WHO Child Growth Standards median. Population of interest: all children below five years old. Authors provided.
To fight against hunger and malnutrition, India has a long history of in-kind social programs, which have been put under the umbrella of the National Food Security Act (also known as the Right to Food Act) in 2013. Given the current emergency, the Central Minister of Finance Nirmala Sitharaman announced measures reinforcing these existing social programs and other schemes a few hours after the lockdown declaration. The package, called the Pradhan Mantri Garib Kalyan Yojana (the Prime Minister’s Poor Welfare Scheme), covers about 21 billion euros. These measures have been critically welcomed by economists. Among them, Jayati Ghosh deemed this scheme “embarrassing” given the small amount put on the table and “inadequate”. The Indian Society of Labour Economics, comprising leading economists, wrote a letter to the Prime Minister and state Chief Ministers and stated that the assistance needed amounted to 434 billion euro, more than 20 times the amount in the planned scheme.
In the announced package, cash support will be set up using existing direct transfer schemes, in particular the Mahatma Gandhi National Rural Employment Guarantee Act (MNREGA), a cash program that provides 100 days of guaranteed paid work for rural dwellers to fight against underemployment. But the announced increase in MNREGA wages is pointed to as just adjusting for an already planned one. [17] This program could benefit internal migrant workers left without economic resources, but only under the condition that they manage to get back home, where they are administratively registered. As for in-kind measures, the government wants to expand the Public Distribution System (PDS), by supporting the main food calorie intakes in India: cereals (more than 50 percent of the total calorie intakes) and pulses (about 12 percent, an important source of protein in a country consuming little animal products). [18] But the promises may not be enough to cover the needs. Officials have also pointed out that this stock will be difficult to deliver since private millers are facing a shortage of labour. [19] Finally, the Mid Day Meal Scheme (MDMS), which provides a free meal to every kid enrolled in schools, is currently stopped despite its critical role in child nutrition (Khera, 2013).
More importantly, the main issues around these measures are existing corruption and exclusion errors, although the PDS is theoretically wide-covering. The ability to target everyone in need is critical in the present situation (the use of a biometric authentication system based, the controversial Aadhaar-Based Biometric Authentication does not seem to solve these problems, Drèze et al., 2017). The economist Jean Drèze has hence advocated for providing food supply in “emergency facilities” to any person without asking for an Aadhar number or ration card.
Facing the emerging crisis, private initiatives from NGOs, organising food points in urban areas, or Sikh temples hosting and feeding the homeless (Parulkar and Naik, 2020), have flourished. Not only has the voluntary sector considerably dried up over the last two decades, but without huge public support, local initiatives will not be sufficient. In Tamil Nadu, those who are still in place have so far mostly been focusing on awareness measures and precautions to be taken to limit the propagation of the virus, raising more suspicion than trust since people’s primary concern is their livelihood. As Jean Drèze warns the government: “Poor people are used to taking a lot of things lying down—when people are hungry and feeble, they are not necessarily well placed to revolt. But food riots could happen, who knows”.
Conclusion
In such a historical moment, one would expect to place national unity above all and to relegate stigmatization as well as religious/ethnic/caste/class-based polarization to the backstage. But nothing is less certain. As migrants go home, they face attacks and are ostracized by fear of infection. And it was not long before hatred discourses surfaced in this crisis with Muslim, north-eastern, tribal or Dalit Indians, all being accused of spreading the virus. [20] It is yet to observe whether and how the government will take the opportunity of this crisis to further divide or re-unite its people. The immediate concern is for the poor and the minorities, who as we have seen, will be the first to suffer from this crisis. For them, the consequences of the lockdown will be dramatic. They will die at home, in silence, maybe from a much deadlier thing than the virus itself: the profound socioeconomic inequalities that divide Indian society.
Given the large diversity of situations on the Indian subcontinent, regional public responses seem more adequate to circumvent the economic and humanitarian tragedy. Several states have been at the forefront implementing ambitious emergency solutions for the most needy, including Kerala, Delhi, Odisha or West Bengal, even though their action is partly withheld by cash transfers from the Central government. The informal sector, though badly hit by the lockdown, has also proved incredibly resilient in past crises and this provides hope in these unprecedented circumstances. In the longer run, investing in the agriculture sector would help regenerate the economy, by ensuring food security and reducing the urban-rural gap, blatantly revealed by the recent mass exodus.
Cover picture by Kailash Mohankar.
Dossier(s) :
Faces of the Pandemic
Faces of the Pandemic
by & & & , 13 April 2020
Share this article
Find us here :


Further reading
• Jan Breman, Labour Bondage in West India: From Past to Present, New-Delhi, Oxford University Press, 2007.
• Veena Das, Affliction: Health, Disease, Poverty, Fordham University Press, 2015.
• Priya Deshingkar and Shaheen Akter. “Migration and Human Development in India’, United Nations Development Programme.” Human Development Reports, Research Paper 13, 2009.
• Jean Drèze, Nazar Khalid, Reetika Khera, Anmol Somanchi, “Pain without gain? Aadhar and food security in Jharkhand”, Economic and Political Weekly, vol. 52, n°50, 2017.
• Jean Drèze and Amartya Kumar Sen, An Uncertain Glory: India and Its Contradictions, Princeton, Princeton Univ. Press, 2013.
• Sarah Hodges, and Mohan Rao (eds), Public Health and Private Wealth: Stem Cells, Surrogates, and Other Strategic Bodies, Oxford University Press, 2016.
• “India Labour Market Update.” Geneva, ILO, 2016
• Reetika Khera, “Mid-Day Meals: Looking Ahead”, Economic and Political Weekly, vol. 48, n° 32, 2013.
• Ashwin Parulkar, Mukta Naik, “A Crisis of Hunger: a ground report on the repercussions of COVID-19 related lockdown on Delhi’s vulnerable populations”, Centre for Policy Research Report, March 27, 2020.
• David Picherit. “Labour Migration Brokerage and Dalit Politics in Andhra Pradesh: A Dalit Fabric of Labour Circulation.” Journal of Ethnic and Migration Studies, 1-17, 2018
• Elena Reboul, Isabelle Guérin, Antony Raj, and G. Venkatasubramanian. 2019. “Managing Economic Volatility. A Gender Perspective.” Working Papers CEB 19-015, ULB.
• Akshay Swaminathan, Rockli Kim, Yun Xu, Jeffrey C Blossom, William Joe, R Venkataramanan, Alok Kumar, S V Subramanian, “Burden of Child Malnutrition in India”, Economic and Political Weekly, vol. 54, n°12, 2019.
To quote this article :
Marine Al Dahdah & Mathieu Ferry & Isabelle Guérin & Govindan Venkatasubramanian, « The Covid-19 Crisis in India. A Nascent Humanitarian Tragedy », Books and Ideas , 13 April 2020. ISSN : 2105-3030. URL : https://booksandideas.net/The-Covid-19-Crisis-in-India
Nota Bene:
If you want to discuss this essay further, you can send a proposal to the editorial team (redaction at laviedesidees.fr). We will get back to you as soon as possible.
You might also like




Footnotes
[1] In 2018, India accounts for a quarter of the global tuberculosis burden with 2,15 millions of active cases, and an estimated total of 450.000 TB related deaths, diabetes, chronic respiratory and cardiovascular diseases were estimated to account for 3%, 11% and 27% of all deaths. Sources : WHO-India Noncommunicable Diseases (NCD) Country Profiles, 2018 and India TB Report 2019 consulted on 04/04/2020. On the malnutrition burden see the detailed analysis provided in the section of this article called Dying of hunger under the lockdown.
[2] See data from the World Bank on Hospital beds (per 1,000 people)
[3] See estimates in Covid-19: When will states run out of beds?
[4] Approximately 90% of the poorest and 67% of the richest urban Indians do not have health insurance according to NSSO 75th round
[5] According to NSSO data, in 2011-12 the agricultural sector accounts for 62.7 per cent of India’s employment, against 77.6% in 1993-94 (ILO, 2016: 2).
[6] Self-consumption, long a pillar of food security for rural families, has declined sharply over the last decades; see the next section.
[7] Schooling rates have risen sharply in recent decades, including for girls, the low castes and Adivasis, and this is to be welcomed, but it entails significant expenses, even when school is free, as a large share remains the responsibility of families (transport, school materials).
[8] Often presented as “unsustainable” or “superfluous” expenses, these expenses turn out to be real investments that make it possible to maintain the social networks that people sorely need to protect themselves.
[9] On 8 November 2016, Indian Prime Minister Narendra Modi announced the impending, almost immediate demonetization of all 500- and 1,000-rupee banknotes and the introduction of a new series of 500 and 2,000-rupee banknotes. See the article from Guérin, Isabelle, Youna Lanos, Sébastien Michiels, Christophe Jalil Nordman, and Govindan Venkatasubramanian. “Insights on Demonetisation from Rural Tamil Nadu.” Economic & Political Weekly 52 (52): 45, 2017.
[10] See Coronavirus: What does it say when PM Modi has to tweet ‘don’t panic!’ after his own speech?
[11] The ‘Consumer Expenditure Survey’ data from the National Sample Survey Office (NSSO) provides the most comprehensive household expenditure data to look at and date back from 2011-2012. Unfortunately, more recent data from the NSSO are not available. Even though a newer household consumption survey was conducted in 2017-2018, the data were never released, despite explicit demands from the research community. The Central government took the pretext of survey instrument biases to never release the complete raw data of the most comprehensive survey to study household consumption in India. But in fact press reports leaked that the total household spendings between the last two surveys fell for the first time in four decades. The impact of the 2016 demonetisation may have affected Indian households’ expenditures on the long run, a point that the government is reluctant to acknowledge. More recent surveys from other institutions do not have the same methodological robustness, geographical coverage, or access to detailed results. These figures are derived from Tables 6C-R and 6C-U p. 106-107 from the report Level and Pattern of Consumer Expenditure 2011-2012.
[12] This figure is based on INSEE estimates from the survey Budget de Famille, 2014.
[14] See P. Sainath’s analysis on the present situation for rural areas, What we should do about COVID-19
[15] Estimates are directly on the Global Hunger Index website, based on a composite indicator associating statistics related to undernourishment, child anthropometric indicators (stunting and wasting) and child mortality.
[19] See Sitharaman’s Promise of Pulses Through PDS Unlikely to See Fruition Anytime Soon. Also read an analysis comparing measure of social distancing and the practice of untouchability: The History of caste has lessons on the dangers of social distancing.
[20] See for instance the controversy around a caricature published in The Hindu, identifying Islamic terrorists with the virus, now taken down, or a Muslim gathering identified as a virus hotspot as analyzed in: It was already dangerous to be Muslim in India. Then came the Coronavirus. See also the account of Muslims beaten up and abused in rural Punjab. A testimony on the rise of stigmatization against North-Eastern people in New Delhi can be read here.
Our partners


Sections
Keep in touch
© laviedesidees.fr - Any replication forbidden without the explicit consent of the editors. - Mentions légales - webdesign : Abel Poucet